I will be talking at the Festival of Genomics on Wednesday 24 January about Identifying virulence and antimicrobial resistance genes in bacterial using genome-wide association studies. You can preview my talk here.
Category Archives: Mycobacterium tuberculosis
New paper: GenomegaMap for dN/dS in over 10,000 genomes
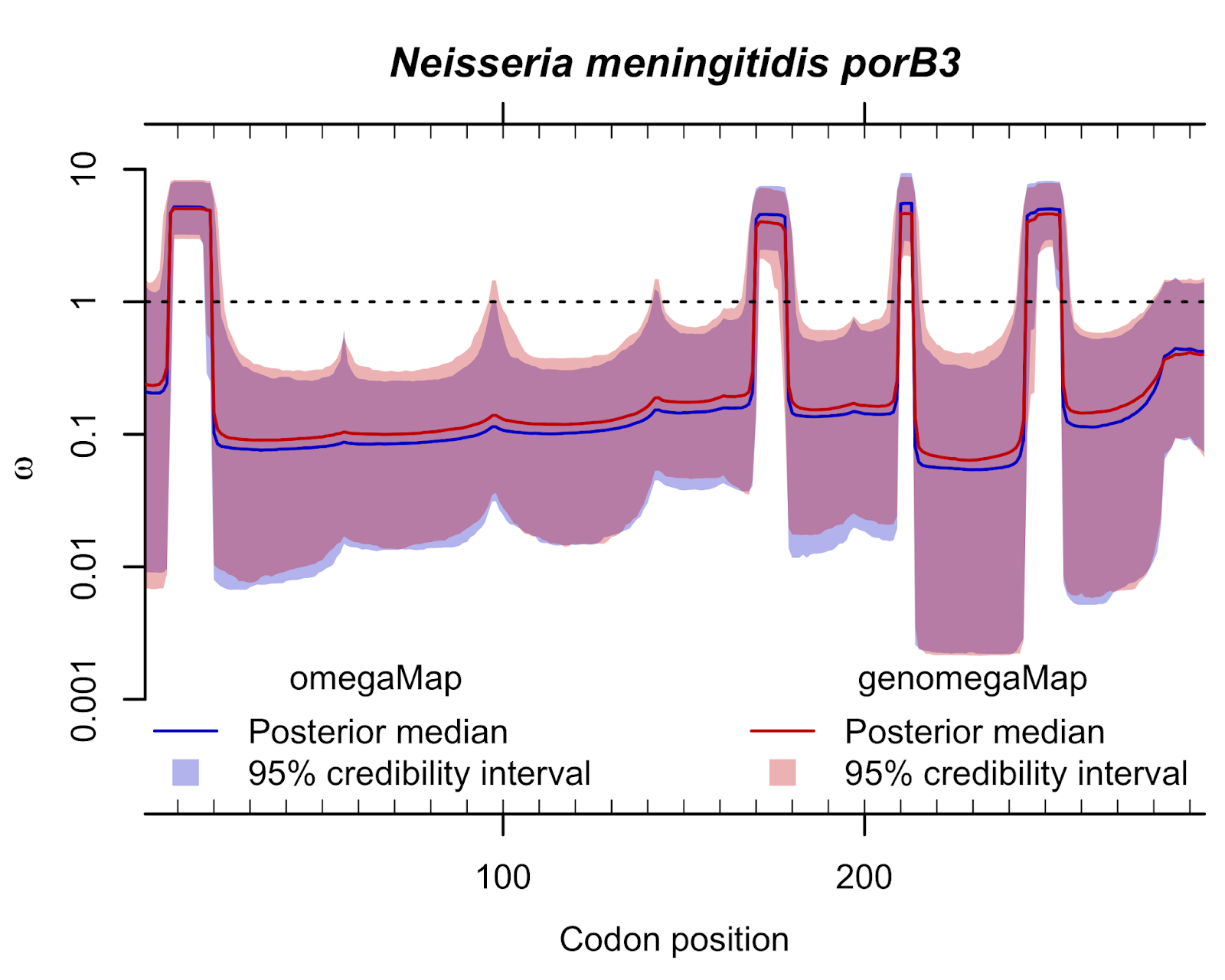 Published this week in Molecular Biology and Evolution, is a new paper joint with the CRyPTIC Consortium "GenomegaMap: within-species genome-wide dN/dS estimation from over 10,000 genomes".
Published this week in Molecular Biology and Evolution, is a new paper joint with the CRyPTIC Consortium "GenomegaMap: within-species genome-wide dN/dS estimation from over 10,000 genomes".The dN/dS ratio is a popular statistic in evolutionary genetics that quantifies the relative rates of protein-altering and non-protein-altering mutations. The rate is adjusted so that under neutral evolution - i.e. when the survival and reproductive advantage of all variants is the same - it equals 1. Typically, dN/dS is observed to be less than 1 meaning that new mutations tend to be disfavoured, implying they are harmful to survival or reproduction. Occasionally, dN/dS is observed to be greater than 1 meaning that new mutations are favoured, implying they provide some survival or reproductive advantage. The aim of estimating dN/dS is usually to identify mutations that provide an advantage.
Theoreticians are often critical of dN/dS because it is more of a descriptive statistic than a process-driven model of evolution. This overlooks the problem that currently available models make simplifying assumptions such as minimal interference between adjacent mutations within genes. These assumptions are not obviously appropriate in many species, including infectious micro-organisms, that exchange genetic material infrequently.
There are many methods for measuring dN/dS. This new paper overcomes two common problems:
- It is fast no matter how many genomes are analysed together.
- It is robust whether there is frequent genetic exchange (which causes phylogenetic methods to report spurious signals of advantageous mutation) or infrequent genetic exchange.
The paper includes detailed simulations that establish the validity of the approach, and it goes on to demonstrate how genomegaMap can detect advantageous mutations in 10,209 genomes of Mycobacterium tuberculosis, the bacterium that causes tuberculosis. The method reproduces known signals of advantageous mutations that make the bacteria resistant to antibiotics, and it discovers a new signal of advantageous mutations in a cold-shock protein called deaD or csdA.
Software that implements genomegaMap is available on Docker Hub and the source code and documentation are available on Git Hub.
With the steady rise of more and more genome sequences, the analysis of data becomes an increasing challenge even with modern computers, so it is hoped that this new method provides a useful way to exploit the opportunities in such large datasets to gain new insights into evolution.
Prize PhD Studentships available
I am offering two PhD projects as part of the annual Nuffield Department of Medicine Prize Studentship competition:
In addition to my projects, the Modernising Medical Microbiology project has announced the following PhD projects as part of the competition:
- Real-time detection of multidrug resistant tuberculosis and transmission in England
Joint with David Wyllie, molecular microbiologist, this project is focused on developing statistical methods for recognizing transmission clusters, integrating genomics approaches with molecular typing schemes and developing future-proof taxonomy for strain identification. - Tracking future infection threats using genomic data and electronic health records
Joint with David Clifton, biomedical engineer, this project aims to develop new machine learning and statistical methods to identify genomic markers of antibiotic resistance and susceptibility within various pathogens, to help track future infection threats.
In addition to my projects, the Modernising Medical Microbiology project has announced the following PhD projects as part of the competition:
- Antimicrobial resistance gene/vector transmission across human, animal and environmental reservoirs
Supervised by Nicole Stoesser, Nicola De Maio and Derrick Crook - Healthcare big data and genomics for infectious disease threat detection
Supervised by David Clifton, David Eyre and Tim Peto - Prediction of Mycobacterium tuberculosis drug resistance through genome sequencing clinical samples
Supervised by Tim Walker and Tim Peto - Antibiotic resistance in Tuberculosis: Predicting de novo the effect of individual genetic mutations
Supervised by Phil Fowler and Sarah Walker
Postdoctoral Scientist in Statistical Genomics
We are recruiting for a Postdoctoral Scientist in Statistical Genomics working on Antimicrobial Resistance (AMR) gene discovery and focused on Tuberculosis. This will be a joint position at the University of Oxford between Derrick Crook's group and mine, and part of the large international CRyPTIC consortium.
The role is for a population geneticist or statistical geneticist to develop and apply statistical methods, including genome-wide association studies, for discovering rare and common genetic variants underlying antimicrobial resistance in Mycobacterium tuberculosis.
One third of the world's population - 2.5 billion people - are thought to be infected with tuberculosis (TB). This post offers an opportunity to work with global TB experts from five continents, statistical geneticists, clinicians, medical statisticians and software engineers; integrating statistical genetics, bioinformatics and machine learning methods with the aim of uncovering all genomic variants causing at least 1% resistance to first line anti-TB drugs.
We're looking for candidates with a PhD in genomics, evolutionary biology, statistics or a related subject. The post is full-time and fixed-term for up to 3 years initially.
The deadline for applications is noon on Friday 6th May 2016.
The role is for a population geneticist or statistical geneticist to develop and apply statistical methods, including genome-wide association studies, for discovering rare and common genetic variants underlying antimicrobial resistance in Mycobacterium tuberculosis.
One third of the world's population - 2.5 billion people - are thought to be infected with tuberculosis (TB). This post offers an opportunity to work with global TB experts from five continents, statistical geneticists, clinicians, medical statisticians and software engineers; integrating statistical genetics, bioinformatics and machine learning methods with the aim of uncovering all genomic variants causing at least 1% resistance to first line anti-TB drugs.
We're looking for candidates with a PhD in genomics, evolutionary biology, statistics or a related subject. The post is full-time and fixed-term for up to 3 years initially.
The deadline for applications is noon on Friday 6th May 2016.
Posted by in Antibiotics, CRyPTIC, Derrick Crook, Genomics, GWAS, Microbiology, Mycobacterium tuberculosis, Population Genetics, Postdoc
Making the most of bacterial GWAS: new paper in Nature Microbiology
In a new paper published this week in Nature Microbiology, we report the performance of genome wide association studies (GWAS) in bacteria to identify causal mechanisms of antibiotic resistance in four major pathogens, and introduce a new method, bugwas, to make the most of bacterial GWAS for traits under less strong selection.
As explained by Sarah Earle, joint first author with Jessie Wu and Jane Charlesworth, the problem with GWAS in bacteria is strong population structure and the consequent strong coinheritance of genetic variants throughout the genome. This phenomenon - known as genome-wide linkage disequilibrium (LD) - comes about because exchange of genes is relatively infrequent in bacteria, which reproduce clonally, compared to organisms that exchange genes every generation through sexual reproduction.
Genome-wide LD makes it difficult for GWAS to distinguish variants that causally influence a trait from other, coinherited variants that have no direct effect on the trait.
In the case of antibiotic resistance - a trait of high importance to human health - bacteria are under extraordinary selection pressures because resistance is a matter of life and death, to them as well as their human host. This helps overcome coinheritance and pinpoint causal variants because antibiotic usage selects for the independent evolution of the same resistance-causing variants in different genetic backgrounds.
Consequently, bacterial GWAS works very efficiently for antibiotic resistance: the variants most significantly associated with antibiotic resistance in 26 out of the 27 GWAS we performed were genuine resistance-conferring mutations. In the 27th we uncovered a putative novel mechanism of resistance to cefazolin in E. coli. These results for 17 antibiotics (ampicillin, cefazolin, cefuroxime, ceftriaxone, ciprofloxacin, erythromycin, ethambutol, fusidic acid, gentamicin, isoniazid, penicillin, pyrazinamide, methicillin, rifampicin, tetracycline, tobramycin and trimethoprim) across four species (E. coli, K. pneumoniae, M. tuberculosis and S. aureus) build on earlier work investigating beta-lactam resistance in S. pneumoniae, and convincingly demonstrate the potential for bacterial GWAS to discover new genes underlying important traits under strong selection.
What about traits under less strong selection, which probably includes pretty much every other bacterial trait? We show in this context that coinheritance poses a major challenge, based on detailed simulations. Often it may not be possible to use GWAS to pinpoint individual variants responsible for different traits because they are coinherited with - possibly many - other uninvolved variants.
But all is not lost. We show that even when individual locus-level effects cannot be pinpointed, there is often excellent power to characterize lineage-level differences in phenotype between strains. This is helpful for multiple reasons: (1) we often conceptualize trait variability in bacteria at the level of strain-to-strain differences (2) these differences can be highly predictive (3) we can prioritize variants for functional follow-up based on their contribution to strain-level differences.
These concepts represent a substantial departure from regular GWAS. In the human setting for instance, lineage-level differences are usually discarded as uninteresting or artefactual, and variants are almost always prioritized based on statistical evidence for involvement over-and-above any contribution to lineage-level differences. In the bacterial setting, we are forced to depart from these conventions because a large proportion of all genetic variation is strongly strain-stratified. To find out more, see the paper and try our methods.
As explained by Sarah Earle, joint first author with Jessie Wu and Jane Charlesworth, the problem with GWAS in bacteria is strong population structure and the consequent strong coinheritance of genetic variants throughout the genome. This phenomenon - known as genome-wide linkage disequilibrium (LD) - comes about because exchange of genes is relatively infrequent in bacteria, which reproduce clonally, compared to organisms that exchange genes every generation through sexual reproduction.
Genome-wide LD makes it difficult for GWAS to distinguish variants that causally influence a trait from other, coinherited variants that have no direct effect on the trait.
In the case of antibiotic resistance - a trait of high importance to human health - bacteria are under extraordinary selection pressures because resistance is a matter of life and death, to them as well as their human host. This helps overcome coinheritance and pinpoint causal variants because antibiotic usage selects for the independent evolution of the same resistance-causing variants in different genetic backgrounds.
Consequently, bacterial GWAS works very efficiently for antibiotic resistance: the variants most significantly associated with antibiotic resistance in 26 out of the 27 GWAS we performed were genuine resistance-conferring mutations. In the 27th we uncovered a putative novel mechanism of resistance to cefazolin in E. coli. These results for 17 antibiotics (ampicillin, cefazolin, cefuroxime, ceftriaxone, ciprofloxacin, erythromycin, ethambutol, fusidic acid, gentamicin, isoniazid, penicillin, pyrazinamide, methicillin, rifampicin, tetracycline, tobramycin and trimethoprim) across four species (E. coli, K. pneumoniae, M. tuberculosis and S. aureus) build on earlier work investigating beta-lactam resistance in S. pneumoniae, and convincingly demonstrate the potential for bacterial GWAS to discover new genes underlying important traits under strong selection.
What about traits under less strong selection, which probably includes pretty much every other bacterial trait? We show in this context that coinheritance poses a major challenge, based on detailed simulations. Often it may not be possible to use GWAS to pinpoint individual variants responsible for different traits because they are coinherited with - possibly many - other uninvolved variants.
But all is not lost. We show that even when individual locus-level effects cannot be pinpointed, there is often excellent power to characterize lineage-level differences in phenotype between strains. This is helpful for multiple reasons: (1) we often conceptualize trait variability in bacteria at the level of strain-to-strain differences (2) these differences can be highly predictive (3) we can prioritize variants for functional follow-up based on their contribution to strain-level differences.
These concepts represent a substantial departure from regular GWAS. In the human setting for instance, lineage-level differences are usually discarded as uninteresting or artefactual, and variants are almost always prioritized based on statistical evidence for involvement over-and-above any contribution to lineage-level differences. In the bacterial setting, we are forced to depart from these conventions because a large proportion of all genetic variation is strongly strain-stratified. To find out more, see the paper and try our methods.
CRyPTIC: rapid diagnosis of drug resistance in TB
The Modernising Medical Microbiology consortium has announced a new worldwide collaboration called CRyPTIC to speed up diagnosis of antibiotic resistant tuberculosis (TB).
TB infects nearly 10 million people each year and kills 1.5 million, making it one of the leading causes of death worldwide. Almost half a million people each year develop multidrug-resistant (MDR) TB, which defies common TB treatments. Time consuming tests must be run to identify MDR-TB and which drugs will work or fail. This delays diagnosis and creates uncertainty about the best drugs to prescribe to individual patients.
CRyPTIC aims to hasten the identification of MDR-TB using whole genome sequencing to identify genetic variants that give resistance to particular drugs. The project is funded by a $2.2m grant from the Bill & Melinda Gates Foundation and a £4m grant from the Wellcome Trust and MRC Newton Fund.
CRyPTIC aims to collect and analyse 100,000 TB cases from across the world, providing a database of MDR-TB that will underpin diagnosis using WGS. Samples from across Africa, Asia, Europe and the Americas will be collected by teams at more than a dozen centres They will conduct drug resistance testing and much of the genome sequencing. Read more information here.
TB infects nearly 10 million people each year and kills 1.5 million, making it one of the leading causes of death worldwide. Almost half a million people each year develop multidrug-resistant (MDR) TB, which defies common TB treatments. Time consuming tests must be run to identify MDR-TB and which drugs will work or fail. This delays diagnosis and creates uncertainty about the best drugs to prescribe to individual patients.
CRyPTIC aims to hasten the identification of MDR-TB using whole genome sequencing to identify genetic variants that give resistance to particular drugs. The project is funded by a $2.2m grant from the Bill & Melinda Gates Foundation and a £4m grant from the Wellcome Trust and MRC Newton Fund.
CRyPTIC aims to collect and analyse 100,000 TB cases from across the world, providing a database of MDR-TB that will underpin diagnosis using WGS. Samples from across Africa, Asia, Europe and the Americas will be collected by teams at more than a dozen centres They will conduct drug resistance testing and much of the genome sequencing. Read more information here.
Identifying and treating latent TB cases is critical for TB elimination

By Paul Zell, specialist, TB Program, APHL
For many in the United States, Mycobacterium tuberculosis (TB) is not a concern. It is viewed as a disease that is uncommon in the US and seldom a real threat to your average person. This could not be further from the truth.
There are two types of TB: TB disease and latent TB infection. A person with TB disease has an active infection, is presenting symptoms and is contagious. A person with latent TB has TB bacteria in their body but doesn’t have any symptoms and therefore is not contagious. However, a person with latent TB can develop TB disease at any point in their life, present symptoms and potentially infect others. Because people with latent TB are asymptomatic, many latent TB infections in the US go undetected.
In 2014, there were nearly 10,000 TB cases reported in the US. Relative to other infectious diseases, 10,000 cases may seem low in a nation of 318.9 million people. However, this number only represents those with active TB disease, not the total number of people who are actually infected with TB. So how do we count the number of people with latent TB infections?
CDC’s Division of TB Elimination (DTBE) estimates that up to 13 million people in the US have latent TB. A study conducted by DTBE suggested that only 11.4% of active TB disease cases are attributed to new infections and that the percentage of infections from latent TB could be as high as 85-90%. So while the number of active TB cases has been declining since its peak in 1992, TB has the potential to become resurgent in the United States through these latent TB cases. Thus the goal of TB elimination in the US can only be realized if latent TB cases are routinely identified and the patients are promptly treated.
 Detecting latent TB infections is critical to TB control efforts. When a person with latent TB is diagnosed, they can be treated prior to becoming symptomatic and infectious. However, because a person with latent TB has no active infection and therefore no symptoms, diagnosing latent TB requires a test or tests that looks for signs that the bacterium has infected the body.
Detecting latent TB infections is critical to TB control efforts. When a person with latent TB is diagnosed, they can be treated prior to becoming symptomatic and infectious. However, because a person with latent TB has no active infection and therefore no symptoms, diagnosing latent TB requires a test or tests that looks for signs that the bacterium has infected the body.
The tuberculin skin test (TST) is the most well-known. Many of you have likely had a TST. You would have received a very small injection under the skin in your forearm and been asked to return to your health care provider’s office a few days later to be checked for an immune response that would appear as an induration (large red blotch).
In addition to the skin test, there is also a newer blood test: the Interferon Gamma Release Assays (IGRA). Much like any other one-time blood test, your health care provider would draw your blood and send the sample to a laboratory for testing. The results would then be communicated to your provider who would share them with you. While this test is most commonly performed by hospital or commercial laboratories, public health laboratories around the nation are working with CDC to increase implementation of IGRA testing to make it more widely available. This expansion will improve the detection, treatment and follow-up of individuals with latent TB infections.
Neither these TB tests are perfect, but together they give us a fundamental toolkit to identify latent TB cases.
This year, the theme of World TB Day is, “United to End TB.” Along with our partners, APHL is working to make “End TB” a reality, not just a campaign slogan. We feel strongly that public health laboratories play a vital role in accomplishing this goal by increasing access to TB testing in the US.
Posted by in All Posts, Infectious Diseases, Latent TB, Mycobacterium tuberculosis, tB, tuberculosis, world tb day
Postdoc in antimicrobial resistance gene discovery
There is an opening for a Postdoctoral Scientist in Microbial Genomics working on Antimicrobial Resistance Gene Discovery and focused on Tuberculosis which is advertised on the University of Oxford website. This will be a joint position with Derrick Crook's group and part of a larger international consortium.
The role is for a population geneticist or statistical geneticist working with TB experts from five continents with the aim of uncovering all genomic variants causing at least 1% resistance to first line TB drugs. We're looking for candidates with a PhD in genomics, evolutionary biology, statistics or a related subject. The post is full-time and fixed-term for up to 3 years initially.
The deadline for applications is noon on Monday 15th February 2016.
The role is for a population geneticist or statistical geneticist working with TB experts from five continents with the aim of uncovering all genomic variants causing at least 1% resistance to first line TB drugs. We're looking for candidates with a PhD in genomics, evolutionary biology, statistics or a related subject. The post is full-time and fixed-term for up to 3 years initially.
The deadline for applications is noon on Monday 15th February 2016.
Posted by in Derrick Crook, Genomics, GWAS, Microbiology, Mycobacterium tuberculosis, Population Genetics, Postdoc
The Tenacity of Tuberculosis: MDR-TB
By William A. Murtaugh, MPH, Specialist, TB Program, APHL
“Suddenly she stopped, clutched her throat and a wave of crimson blood ran down her breast… It rendered her even more ethereal.” ~ Edgar Allan Poe describes his wife dying of tuberculosis.
Disturbing, sensational and oddly romanticized — these were the days of tuberculosis past. So what has become of its future?

While recent news stories about en vogue infectious diseases are no less sensational, TB has certainly lost its status at the water cooler. It is far from having the mystique of a zombie apocalypse; it’s not wrapped up in a passionate human rights movement like HIV/AIDS; it doesn’t have the exotic novelty of Ebola; and it hardly provokes the Thought Police like vaccine preventable diseases. With a low burden of disease in the US and case rates continuing to decline annually, TB has all but faded from public consciousness.
But what TB has lost in zeitgeist influence, it has made up for in tenacity. For every major advancement in treatment and control, M. tuberculosis has capitalized on weaknesses and dared the public health system to rest on its laurels. As a result, the US, a country with relatively robust TB control programs, has not achieved TB elimination. Globally, large disparities in resources and infrastructure remain and TB is the second largest cause of mortality of any single pathogen behind HIV.
In the US, TB often persists in marginalized and invisible populations such as homeless or foreign-born communities. With few exceptions, cases of TB are still reported by every state. Occasionally, rare outbreaks breach the imaginary safety bubble of larger communities. It is vital to recognize that our current system is neither infallible nor exclusive of the global TB fight. The TB of today poses a challenge that could take the hot air from the lungs of the most bumptious pathogen pundit. That threat, and this year’s topic for World TB Day, is multi-drug resistant tuberculosis (MDR-TB).
Multi-drug resistant tuberculosis is defined as active disease from infection by M. tuberculosis strains that are resistant to at least rifampin and isoniazid, two of the four drugs in first line drug therapy (collectively and colloquially known by the acronym “RIPE”). The reasons that TB strains develop drug resistance are complicated and derive from a variety of biological and man-made influences. The major concern with MDR-TB is that it renders inadequate an already limited number of drugs, with only prolonged, less effective and more toxic treatment options remaining.
The story of MDR-TB has its roots right here on, or rather in, our soil. Streptomycin, the first drug to treat TB, is an antibiotic produced by bacteria found in the soil, and is a Nobel Prize winning discovery by Selman Waksman of Rutgers University. While blindingly obvious, drug resistance can’t develop without one key component…drugs. But drug resistant TB was unheard of prior to the discovery of streptomycin in 1943. Not to be outdone, M. tuberculosis showed that it could quickly develop resistance. Through the next 20 years this TB tit-for-tat went on with each newly developed drug until a regimen of combination therapy, the RIPE panel of drugs, provided the TKO and is still the primary arsenal used today. This drug regimen was lengthy with harsh side effects, but it was nonetheless effective. US case rates began to decline through the 1970s. However, the silver bullet of antituberculosis drug discovery was a silver lining that encircled a menacing storm cloud of emerging drug resistant TB.
Optimism in new treatment regimens gave way to the reality that global scale-up of effective treatment programs was a long term investment and expensive. Funders wanted the most bang for their buck, and TB didn’t fit the bill. Consequently, global political will eroded and only wealthy countries, like the US, made significant strides toward TB elimination. Low resource, high burden countries faced limited access to antituberculosis drug supplies and deficient healthcare infrastructure. This contributed to the improper use of drugs that consequently encouraged the emergence of resistant TB strains and subsequent outbreaks of multi-drug resistant TB. These factors led to treatment failure and widespread transmission, and paved a road for outbreaks of multi-drug resistant TB.
Not until the 1990s, when TB remained the single largest cause of death from an infectious disease, were advances made in public health economics that supported investment in TB treatment efforts. The World Health Organization implemented a strategy that is the foundation of today’s approach: Directly Observed Therapy short-course (DOTS). DOTS strategy, as the name indicates, involves a high level of accountability for treatment adherence. Unfortunately, drug resistant strains of M. tuberculosis cannot be determined through direct observation or even under a microscope. MDR-TB patients were failed by the original DOTS strategy because it did not include a significant laboratory component to detect drug resistance. This weakness, coupled with comorbidity associated with a mounting HIV epidemic, gave rise to numerous MDR-TB outbreaks here in the US.
Traditional methods for TB drug susceptibility testing in the laboratory greatly improve the ability to properly treat and control MDR-TB, but require weeks of precious time and expertise. This often limits their utility. The Centers for Disease Control and Prevention Division of TB Elimination, in conjunction with APHL and state and local public health laboratory systems in the US, continue to play an important role in maintaining expertise amid overall declining rates of TB. Great strides have been made in the past decade in development and implementation of technologies that can inform treatment decisions within 24 hours and in greater detail than was ever thought possible.
With a bolster to the domestic diagnostic infrastructure, MDR-TB cases are able to be detected and remain rare (95 cases in 2013). But MDR-TB is showing little sign of significant decrease and, as of 2013, nearly 90% of cases were foreign-born. While barely registering in headlines, MDR-TB is nevertheless the next major obstacle to tuberculosis control. Its path will determine global progress toward TB elimination.
Check out APHL’s webinars related to TB:
- TB and TB Laboratory Assays in the 21st Century: Get an overview about the tuberculosis epidemic in the United States and abroad as well as the various laboratory assays performed to diagnose tuberculosis.
- Mycobacteria Susceptibility Testing: Learn how to best integrate real-time PCR methods, DNA sequencing and culture-based drug susceptibility testing to guide TB treatment.
- Nontuberculous Mycobacteria (NTM) – a New Exciting World: This webinar will discuss current methods to identify NTM and to determine their antimicrobial drug susceptibility.
Posted by in Infectious Diseases, Mycobacterium tuberculosis, tB, World Tuberculosis Day