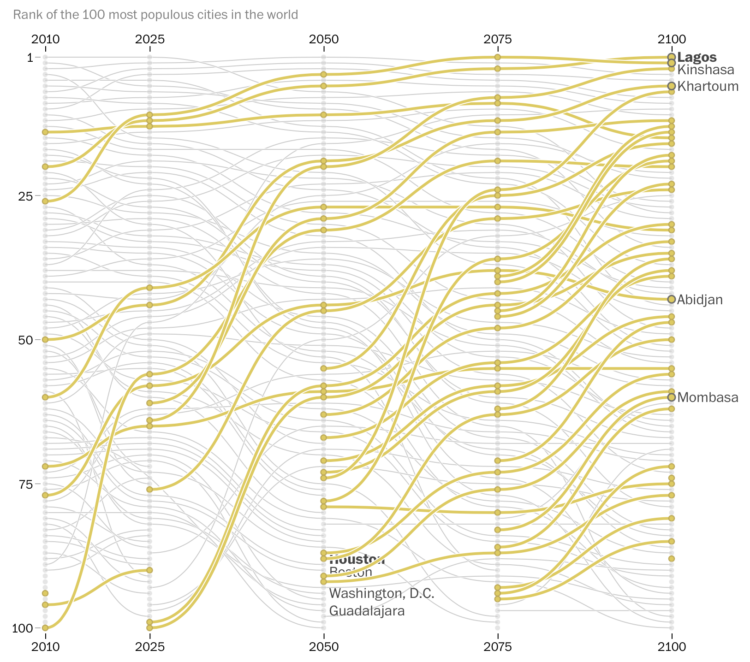
In three projections by the University of Toronto’s Global Cities Institute, Africa accounted for at least 10 of the world’s 20 most populous cities in 2100. Even in the institute’s middle-of-the-road development scenario, cities that many Americans may seldom read about, such as Niamey, Niger, and Lusaka, Zambia, eclipse New York City in growth.
Many U.S. cities such as Atlanta, Houston, and Washington, D.C. are projected to fall out of the top 100 by 2100.
Countries in Africa are no strangers to major disease outbreaks that can result in illness and death of millions of people. In the past two years alone the continent has experienced infectious disease outbreaks of cholera, meningitis, Ebola Virus Disease, Lassa fever, and Yellow fever, and other public health emergencies such as drought and famine.
Understanding the big picture
Training participants from Zanzibar discuss the development of an emergency management program.
It is vitally important to have a big picture perspective on emergency management and response – if one country is not prepared for a public health emergency, then all the countries in the region are susceptible to public health threats that can easily cross borders and impact surrounding countries. This is where public health emergency management (PHEM) comes in. In-country PHEM capacities and systems can be strengthened to support global health security. When the workforce is trained, emergency management infrastructure is in place, and functional systems exist, a country is better positioned to execute a coordinated response that can mitigate risk and save lives.
CDC and other international partners support ongoing efforts to help countries across Africa build capacity in outbreak detection and response. This includes preventing avoidable epidemics, detecting public health threats early, and responding rapidly and effectively to outbreaks of international concern. CDC provides expertise in PHEM to train emergency management technicians, provide input on emergency management operations, and guide development of functional processes and systems for ministries of health around the globe.
Getting the workforce ready to respond
In August 2017, CDC spearheaded a 5-day PHEM workshop in partnership with the World Health Organization, the United States Defense Threat Reduction Agency, and Public Health England. The workshop brought together 55 emergency management staff members from across Africa to learn from experts in the field about how to enhance coordination and response capabilities of their country’s PHEM programs.
Participants came from seven countries – Tanzania, Uganda, Kenya, Ethiopia, Liberia, Sierra Leone, and Nigeria – which all share common interests and challenges related to emergency response. The training focused on developing core principles in PHEM, including trained staff, physical infrastructure, and processes to run a fully functional Public Health Emergency Operations Center (PHEOC). The training highlighted best practices, but since many of the participants had first-hand accounts of responding to public health events in their own countries, they were encouraged to share experiences and network with their peers.
Sharing knowledge and expertise
Public health professionals who work in emergency response know that it’s important to build relationships before an incident so that during a response you work effectively and efficiently with partners. One participant noted that the “rich, valuable contributions from other people’s experiences to build upon what I already knew” was one of the most rewarding parts of the workshop.
The tabletop exercises at the end of the workshop emphasized the importance of information and idea sharing. Participants engaged in tabletop exercises that simulated a response to a Yellow Fever outbreak in northern Tanzania. Participants were divided into 7 teams: management, plans, logistics, operations, finance and administration, communication, and partners. Each team had a mix of participants from different countries. Teams utilized information they had learned throughout the workshop to developed response products, including an organizational structure chart, objectives for the response, and an initial situation report. This exercise led to a robust conversation about different approaches to public health emergency response.
Seeing response in action
Public Health Emergency Operations staff survey the scene after mudslides in Regent, Sierra Leone.
A highlight of the training was when Dr. Ally Nyanga, the Tanzania Ministry of Health PHEOC Manager and an alumni of the CDC Public Health Emergency Management Fellowship, took workshop participants on a tour of the Tanzania PHEOC, a small room on the third floor of the Ministry of Health building. Previously used as a storage area for the library, the 10 x 20 foot PHEOC is now an efficient space that staff can use when they respond to public health emergencies and outbreaks. To date, Tanzania’s PHEOC has been activated to respond to widespread cases of Aflotoxicosis, a type of severe food poisoning, and cholera outbreaks in Tanzania.
While the workshop is over and participants have returned home, the work that they do to prepare for the next public health emergency is ongoing. The workshop highlighted some important takeaways – you do not need a big space and high-tech equipment to respond quickly and efficiently to a public health emergency. Instead, coordination to share information, resources, and ideas is vital to a successful emergency response, both in-country and across an entire region.
0000-0002-8715-2896 Oldest Homo sapiens a “nothingburger”? Plus top journos blast secrecy on health care law Posted June 16, 2017 by Tabitha M. Powledge in Uncategorized post-info AddThis Sharing Buttons above OLDEST HOMO SAPIENS? It’s
0000-0002-8715-2896 Like many scientists, Jean-François Bastin and colleagues had a question. A question that on its surface seems like it may have an obvious answer, or at least, an obvious way to find out the
0000-0002-8715-2896 News about ancient humanity: Humans in California 130,000 years ago? Homo naledi find is much younger than expected Posted May 5, 2017 by Tabitha M. Powledge in Uncategorized post-info AddThis Sharing Buttons above
0000-0002-8715-2896Source: Opinion: Who should lead WHO? 0000-0002-8715-2896 The views expressed in this blog post belong solely to its author and do not necessarily reflect the views of PLOS or the PLOS journals. By Zaeem
By Jennifer Dias As social animals, humans often coordinate their lives around cultural norms, formally sanctioned rules that prescribe or proscribe certain behavior. Typically, when a large majority of people are dissatisfied with an existing
Throughout the month of December, Public Health Matters is conducting a series of year-in-review posts of some of the most impactful disease outbreaks of 2015. These posts will give you a glimpse of the work CDC is doing to prevent, identify, and respond to public health threats.
Getting to Zero
Getting to Zero was a theme and goal that dominated much of CDC’s attention in 2015. In January 2015, The World Health Organization reported that the Ebola epidemic had reached a turning point with the most impacted countries, Liberia, Guinea and Sierra Leone, seeing declines in the number of new cases of Ebola. This turning point came after a year of battling the worst Ebola outbreak in history—resulting in over 20,000 cases by December 2014.
While the spread of the disease and U.S. media attention was at its peak in 2014, some of CDC’s most impactful and important work took place in 2015. This year’s response to the Ebola epidemic was marked with many challenges and accomplishments, new discoveries, and continuous hard work by hundreds of CDC staff. The dedication of CDC and its partners throughout the year has also led to the successful end of widespread Ebola transmission in Liberia and Sierra Leone.
Ebola Vaccine Trials
In April 2015, CDC, in partnership with The College of Medicine and Allied Health Sciences, University of Sierra Leone, and the Sierra Leone Ministry of Health and Sanitation, began a clinical trial to test the potential of a new vaccine to protect against the Ebola virus. This vaccine trial, known as Sierra Leone Trial to Introduce a Vaccine against Ebola (STRIVE), is designed to help protect against Zaire ebolavirus, the virus that is causing the current outbreak in West Africa.
“A safe and effective vaccine would be a very important tool to stop Ebola in the future, and the front-line workers who are volunteering to participate are making a decision that could benefit health care professionals and communities wherever Ebola is a risk,” said CDC Director Tom Frieden, M.D., M.P.H. “We hope this vaccine will be proven effective but in the meantime we must continue doing everything necessary to stop this epidemic —find every case, isolate and treat, safely and respectfully bury the dead, and find every single contact.”
This vaccine trial, along with a series of other vaccine trials taking place in West Africa, represents an important step in the response to the Ebola epidemic. In addition to the tireless efforts being made to completely eliminate Ebola cases, efforts to discover a vaccine could prevent an outbreak of this size in the future.
Leaving Lasting Infrastructures for Health
Programs like STRIVE seek to contribute not only to the future of Ebola prevention research, but also to the future of health care capabilities in the areas impacted by the Ebola epidemic. The STRIVE study is strengthening the existing research capacity of institutions in Sierra Leone by providing training and research experience to hundreds of staff to use now and for future studies.
CDC is leaving behind newly created emergency operation centers (EOC) in countries affected by widespread Ebola outbreaks. The ministries of health will fully lead these new EOCs, which will provide a place to train healthcare workers to be better prepared to conduct outbreak surveillance and response.
Additionally, 2015 brought the official announcement of plans to create the African Centres for Disease Control and Prevention (African CDC). First proposed in 2013, the African CDC will seek ongoing collaboration with other public health entities across the continent and the world to elevate health outcomes for all citizens. Partners will assist by implementing activities, supporting the establishment of regional collaborating centers, advising the African CDC leadership and staff, and providing technical assistance.
Celebrate the Successes, Look to the Future
2015 brought significant progress in the Ebola response. Yet, while the successes and improvements made to public health infrastructure in West Africa are important to celebrate, the work continues to get to zero and end the largest Ebola outbreak in history.
As we draw closer to our goal of zero cases of Ebola, we are reminded of how critical it is to identify, prevent, and respond to outbreaks to prevent future epidemics of this magnitude.
Most travelers to Africa know to protect themselves from malaria. But malaria is far from the only mosquito-borne disease in Africa. Recent studies have revealed that dengue, a disease that is well recognized in Asia and the Americas, may be commonly misdiagnosed as malaria in Africa. So if you’re traveling to Africa, in addition to taking anti-malarial medications you should also take steps to avoid dengue.
Dengue is a mosquito-transmitted illness that is recognized as a common illness throughout Southeast Asia and much of the Americas. In fact, a study published in 2013 estimated that 390 million dengue virus infections occurred throughout the tropics in 2010. Although 70% of infections were predicted to have occurred in Southeast or Southcentral Asia, the next most affected region (16% of infections) was Africa, followed by the Americas (14% of infections). The large estimated burden of dengue in Africa came as a surprise to some, since dengue is not often recognized to be a risk in Africa.
Dengue is Hard to Diagnose in Africa
There are several reasons why dengue has limited recognition in Africa. First, the lack of laboratory-based diagnostic testing leads to many patients not being diagnosed with dengue. This can be perilous because without early diagnosis and appropriate clinical management, dengue patients are at increased risk for poor outcome. However, in order for a clinician to request dengue testing, they must first be aware of the risk for dengue. This awareness usually comes in the form of a positive diagnostic test result. Hence, without testing there is limited clinical awareness, and without clinical awareness there is limited testing.
Finding Dengue in Africa
Brown indicates countries in which dengue has been reported in residents or returned travelers and where Aedes aegypti mosquitoes are present. Light brown indicates countries where only Ae. aegypti mosquitoes have been detected.
How do we know that there actually is dengue in Africa? First, since 1960 at least 15 countries in Africa had reported locally-acquired dengue cases. In addition, travelers returning home with dengue had been detected after visiting more than 30 African countries. Still more African countries are known to have the Aedes mosquitos that transmit the 4 dengue viruses. These findings together provide strong evidence that dengue is a risk in much of Africa.
Thus, it was not a surprise in the summer of 2013 when dengue outbreaks were detected in several sub-Saharan African countries. In many cases, detection of dengue was facilitated by the availability of rapid dengue diagnostic tests that enabled on-site testing.
Dengue Field Investigations in Angola and Kenya
In a past blog I described the initial findings of a dengue outbreak in Luanda, Angola, in west-central Africa outbreak: dengue cases were initially identified with a rapid diagnostic test and confirmatory diagnostic testing and molecular epidemiologic analysis performed as CDC demonstrated that the virus had actually been circulating in the region for at least 45 years. This provided strong evidence that dengue was endemic in the area. During the outbreak investigation, CDC and the Angola Ministry of Health conducted house-to-house surveys wherein blood specimens and questionnaires were collected. Of more than 400 participants, 10% had been recently infected.
Teams from the Angola Ministry of Health conduct a dengue serosurvey in Mombasa, Luanda. Image courtesy of the Angola Field Epidemiology Training Program.
Though nearly one-third reported recently dengue-like illness, and half had sought medical care, none of the patients with laboratory evidence of infection with dengue virus had been diagnosed with dengue, including one person who had symptoms consistent with severe dengue. Although this investigation yielded more questions than answers, it was clear that there was much more dengue in Luanda than was being recognized clinically. By improving clinical awareness through training of clinicians and strengthening disease surveillance, the ability for diagnosis of individuals ill with dengue or other emerging infectious diseases was improved.
On the opposite coast of Africa in Mombasa, Kenya, although dengue outbreaks had been reported for decades, the first outbreak to be confirmed with laboratory diagnostics occurred in the early 1980s. When an outbreak of non-malarial illness was reported in 2013, blood specimens were sent to a laboratory at Kenya Medical Research Institute (or KEMRI) to determine the cause of the outbreak. Three out of the four dengue viruses were detected during this outbreak, which alone suggested that dengue was endemic in the area. To get a better idea for how much dengue there was in Mombasa, CDC and the Kenya Ministry of Health conducted a representative survey in a populous neighborhood of Kenya. Over 9 days, 1,500 people were enrolled in the serosurvey and testing revealed that 13% of participants were currently or recently infected with a dengue virus. Nearly half of infected individuals reported a recent dengue-like illness, most of which had sought medical care.
Field workers from CDC and the Kenya Ministry of Health conduct a dengue serosurvey in Mombasa, Kenya. Image courtesy of Dr. Esther Ellis.
However, nearly all patients had been diagnosed with malaria. Because Mombasa is a port city that is also popular tourist destination, not only was the apparent magnitude of the outbreak a concern for patient diagnosis and care in Mombasa, it also meant that visitors to Mombasa may not be aware of the risk of dengue and therefore could be getting sick and/or bringing the virus home with them.
What next?
There is not yet a vaccine to prevent infection or medication to treat dengue. Unlike the night-time biting mosquitoes that transmit malaria, the Aedes mosquitoes that spread dengue are day-time biters. Consequently, both residents of and travelers to Africa should protect themselves from mosquito bites to avoid dengue by using mosquito repellent. Other strategies, like staying in places with air conditioning and screens on windows and doors and wearing long sleeve shirts and pants, can also help whether you’re traveling to Africa or other regions of the tropics. For clinicians, if travelers recently returned from Africa with acute febrile illness, consider dengue as a potential cause of the patient’s illness.
We still have much to learn about dengue in Africa, but learning where there is risk of dengue is the first step to avoiding it.




 0000-0002-8715-2896 Oldest Homo sapiens a “nothingburger”? Plus top journos blast secrecy on health care law Posted June 16, 2017 by Tabitha M. Powledge in Uncategorized post-info AddThis Sharing Buttons above OLDEST HOMO SAPIENS? It’s
0000-0002-8715-2896 Oldest Homo sapiens a “nothingburger”? Plus top journos blast secrecy on health care law Posted June 16, 2017 by Tabitha M. Powledge in Uncategorized post-info AddThis Sharing Buttons above OLDEST HOMO SAPIENS? It’s 0000-0002-8715-2896 Like many scientists, Jean-François Bastin and colleagues had a question. A question that on its surface seems like it may have an obvious answer, or at least, an obvious way to find out the
0000-0002-8715-2896 Like many scientists, Jean-François Bastin and colleagues had a question. A question that on its surface seems like it may have an obvious answer, or at least, an obvious way to find out the 0000-0002-8715-2896 News about ancient humanity: Humans in California 130,000 years ago? Homo naledi find is much younger than expected Posted May 5, 2017 by Tabitha M. Powledge in Uncategorized post-info AddThis Sharing Buttons above
0000-0002-8715-2896 News about ancient humanity: Humans in California 130,000 years ago? Homo naledi find is much younger than expected Posted May 5, 2017 by Tabitha M. Powledge in Uncategorized post-info AddThis Sharing Buttons above 0000-0002-8715-2896Source: Opinion: Who should lead WHO? 0000-0002-8715-2896 The views expressed in this blog post belong solely to its author and do not necessarily reflect the views of PLOS or the PLOS journals. By Zaeem
0000-0002-8715-2896Source: Opinion: Who should lead WHO? 0000-0002-8715-2896 The views expressed in this blog post belong solely to its author and do not necessarily reflect the views of PLOS or the PLOS journals. By Zaeem By Jennifer Dias As social animals, humans often coordinate their lives around cultural norms, formally sanctioned rules that prescribe or proscribe certain behavior. Typically, when a large majority of people are dissatisfied with an existing
By Jennifer Dias As social animals, humans often coordinate their lives around cultural norms, formally sanctioned rules that prescribe or proscribe certain behavior. Typically, when a large majority of people are dissatisfied with an existing
 “A safe and effective vaccine would be a very important tool to stop Ebola in the future, and the front-line workers who are volunteering to participate are making a decision that could benefit health care professionals and communities wherever Ebola is a risk,” said CDC Director Tom Frieden, M.D., M.P.H. “We hope this vaccine will be proven effective but in the meantime we must continue doing everything necessary to stop this epidemic —find every case, isolate and treat, safely and respectfully bury the dead, and find every single contact.”
“A safe and effective vaccine would be a very important tool to stop Ebola in the future, and the front-line workers who are volunteering to participate are making a decision that could benefit health care professionals and communities wherever Ebola is a risk,” said CDC Director Tom Frieden, M.D., M.P.H. “We hope this vaccine will be proven effective but in the meantime we must continue doing everything necessary to stop this epidemic —find every case, isolate and treat, safely and respectfully bury the dead, and find every single contact.”




